Population health management is about organizing system in place to manage population proactively and deliver the highest quality care while reducing the cost of engaging patients. This article explains about the basics of Population Health Managementand its success.
Population Health Management (PHM)
With the most advanced and sophisticated healthcare system in the world, the USA might be the most expensive medical care destination. But their expenditure is healthcare is skyrocketing due to lack of access to healthcare for many and gaps in the care provided. Experts in healthcare economy express the need for an organized healthcare reform focusing on making health care more affordable, accessible and delivering high-quality care for all the citizens in the USA.
Healthcare reform- The need for PHM
The first step towards the reform was HITECH Act of 2009 which authorized $19 billion in federal subsidies to physician and hospitals for the Meaningful Use of electronic health records. The Patient Protection and Affordable Care Act of 2010 encouraged providers to responsibility for the cost and quality of care. The Centers for Medicare and Medicaid Services (CMS) were instructed to create a shared savings program for accountable care organizations (ACOs). ACOs are groups of physicians and hospitals dedicated to reducing the heath care cost and to improve the quality of care. As per this program, which began on Jan. 1, 2012, federal government will penalize hospitals for avoidable readmissions and base a portion of their reimbursement on quality measures.
The entire objective of the reform is to move to pay-for-performance from fee-for-service, which is considered as a major reason for cost in U.S.Healthcare system. With the initial success of Patient-Centered Medical Homes (PCMHs) and Accountable Care Organizations (ACOs) models, the reimbursement system is likely to replace fee-for-service. The current shift in healthcare systems will involve increased financial and clinical accountability. Thus, the healthcare system in the US is opting for “population health management" - An approach to providing affordable, quality healthcare and reduce the healthcare cost.
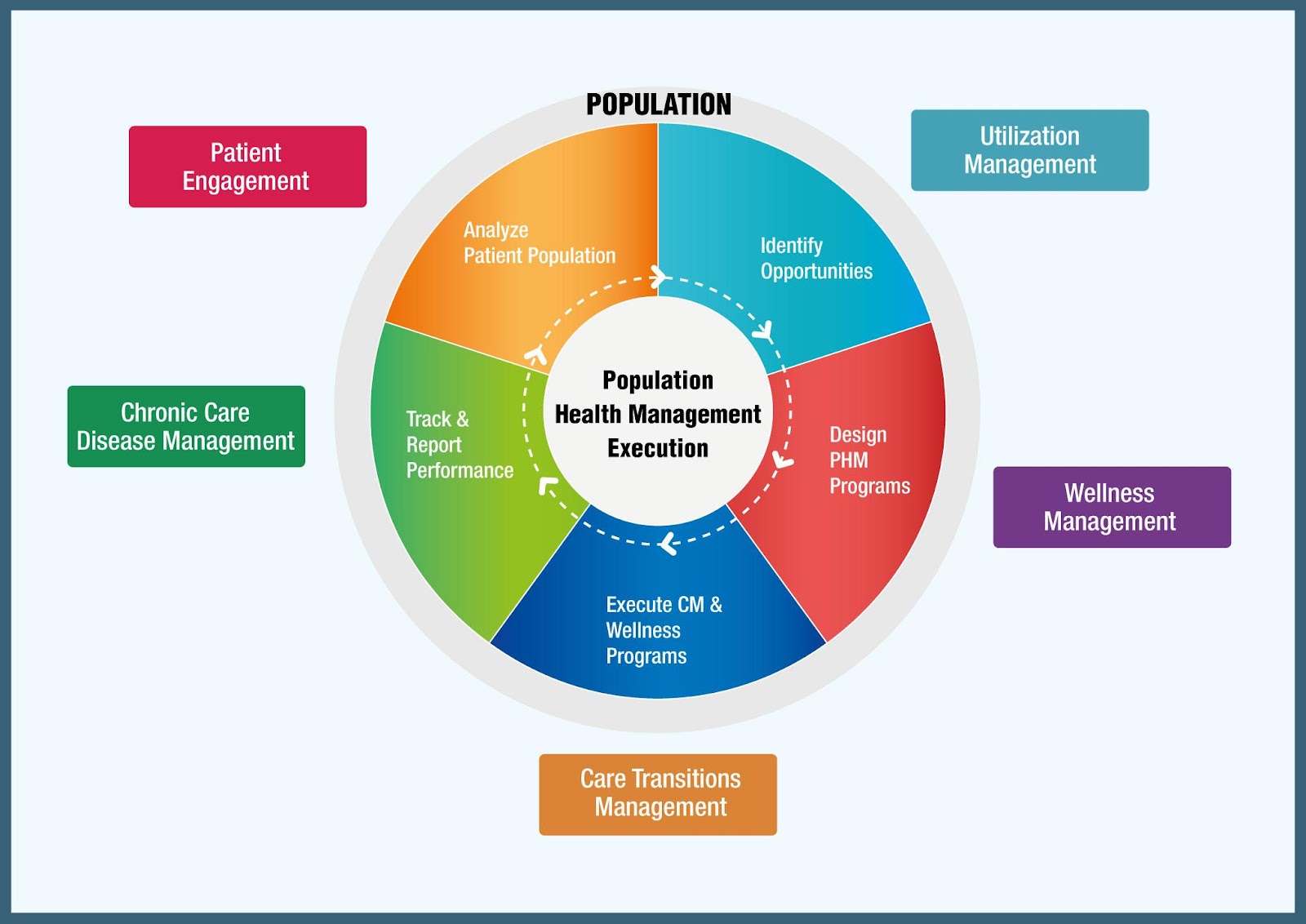
The aim of population health management (PHM) is to keep the patient population healthy, minimizing their encounter with emergency department, hospitalizations, and procedures. It helps to redefine care delivery paradigm from a disease-specific approach to patient-centric approach. To meet its objective, PHM requires automation across the continuum of care to access population needs and stratifying risk based on patient risk arrived by analyzing clinical and non-clinical data.

Successful Implementation of PHM Program
A PHM program, implemented successfully, can work wonders in cutting down the healthcare expenditure and improving your patient’s health outcomes. The following five steps will help providers in planning for successful implementation of PHM program.
DATA is the ‘IT’ thing
Data is the heart and soul of PHM. The healthcare system yields a huge volume of data, at every touch point, from a patient-physician visit to discharge, from medication to health message alerts, from billing to insurance department. These data sets, generated at different levels of care, are just dots. The first step towards implementing PHM begins with connecting these dots by acquiring, aggregating, and leveraging clinical data across the care network. The PHM system demands an efficient data collection, storage, and 360° automation. This implies that we think beyond EHR and its interoperability with other systems. Efforts to make the EHR more sophisticated for data capturing at all levels may be worth exploring.
Analyze the population data:
Data without actionable insight is a waste. Analytics helps in giving insights into the population health status which is the core of any successful PHM program. Algorithms, designed using risk scores using clinical data from electronic medical records and claims, may help to predict vulnerable population.
Supported by non-clinical scores such as compliance, access-to-care and socio-economic, these analytics may help to identify the patients who have a high risk of being hospitalized or likely to have an expensive intervention. The data analysis may facilitate complex tasks such as tracking of the health status of patients, reminding them about medications, and warning them about the risks associated. These interventions may ultimately result in improved patient outcomes, contributing to treatment success.
Bridging the care gaps
There could be many differences or gaps in care, when utilization of health care is compared to the distribution of healthcare, when the treatments provided are compared to the treatment outcomes, when the treatment ordered is compared to the treatment instituted. Care gaps can occur at any level of healthcare, due to numerous reasons. These gaps in care may adversely affect the healthcare costs and the patient health outcomes.
The patient clinical data and utilization pattern, captured through a PHM program, is used to determine whether the patient has a gap in care. Based on this analysis, the care manager designs personalized a care management program to engage at-risk patients in receiving necessary services, alerts, and reminders at the point of care.
Engage your patients for better health outcomes:
Population health solution strives to engage patients at various touch point along with physicians and other clinicians. To optimize the patient engagement, the physicians and care coordinators must be in constant touch with their patients, even if they are out-of-the-hospital. Contact can be established and maintained by sending reminders to the patient's mobile phones, delivering e-mails, or placing a call. However, new technologies like telehealth devices seem to be a great promise. Using these devices, the physician can analyze the telemonitoring data and prescribe preventive and curative measures.
Empower and support the primary care physicians
Primary care physicians (PCPs) are the first point of care for most patients. Therefore, it is important to empower the PCP to ensure that patients receive appropriate and timely care. However, due to shortage of PCPs, formation of a care team, consisting of physicians, nurse practitioners, medical assistants, dietitians, physical therapists, care managers, health coaches, or other professionals, may be needed. The objective is to manage more patients and address their needs timely and efficiently.
The health care system in U.S. is a one-to-one effort, that is, the patient consults the provider even for an insignificant query. But, in the near future, the workflow might change to include phone visits, e-mail consultations, group visits, and encounters with a variety of care team members. This would then reduce the number of hospital visits, thereby benefitting both the PCPs and the patients.